
A 47-year-old overseas Pakistani patient arrived at The Dental Clinic having already researched treatment options across multiple countries. He came with a completely failing dentition across both jaws, active infection at multiple sites, and less than a week before he needed to fly back abroad. Most clinics would have told him to come back in three months.
Under the care of Dr. Saqib Minhas, one of Karachi’s leading implantologists with over 16 years of surgical experience, the case was assessed, planned, and executed within that window.
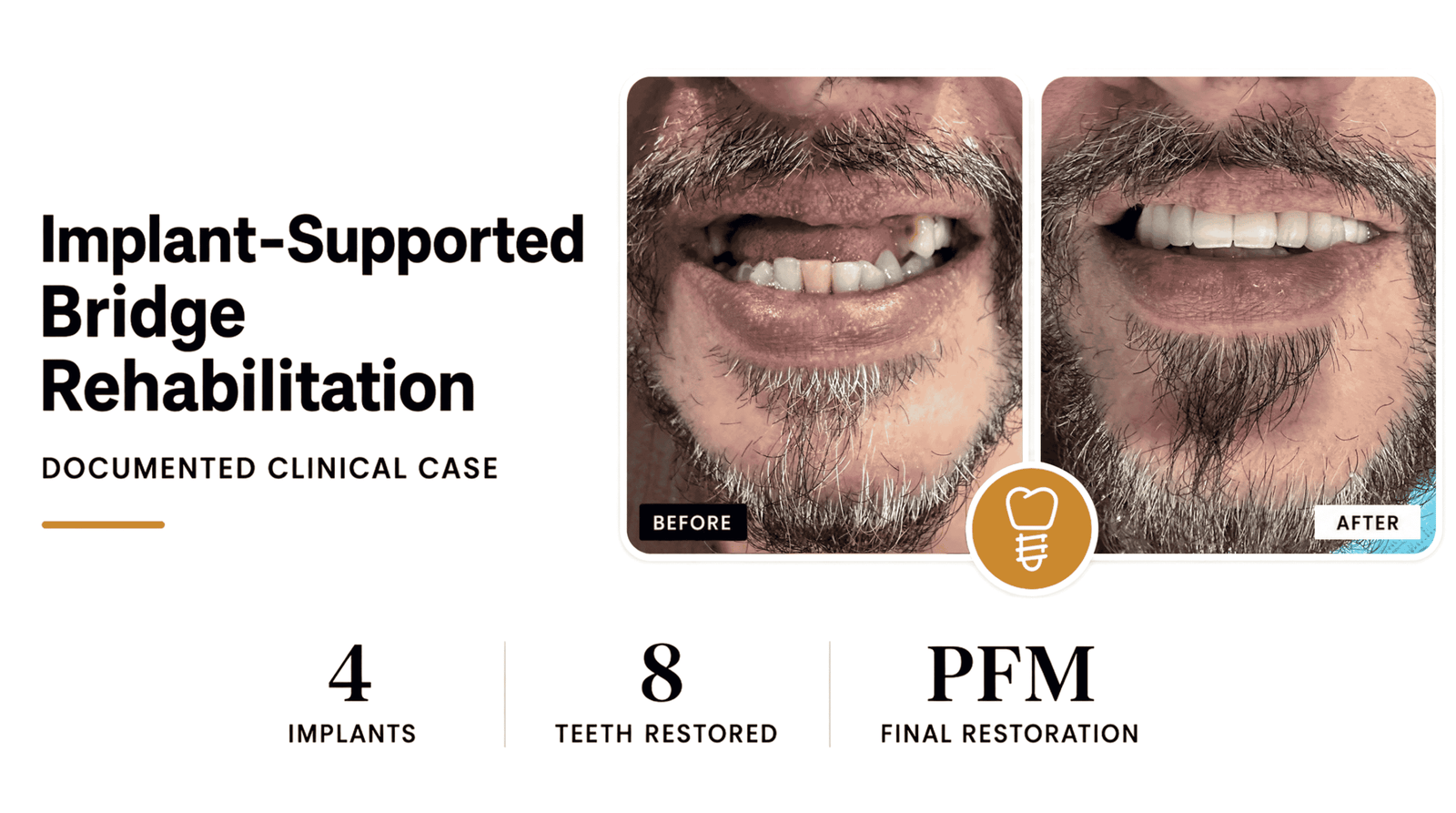
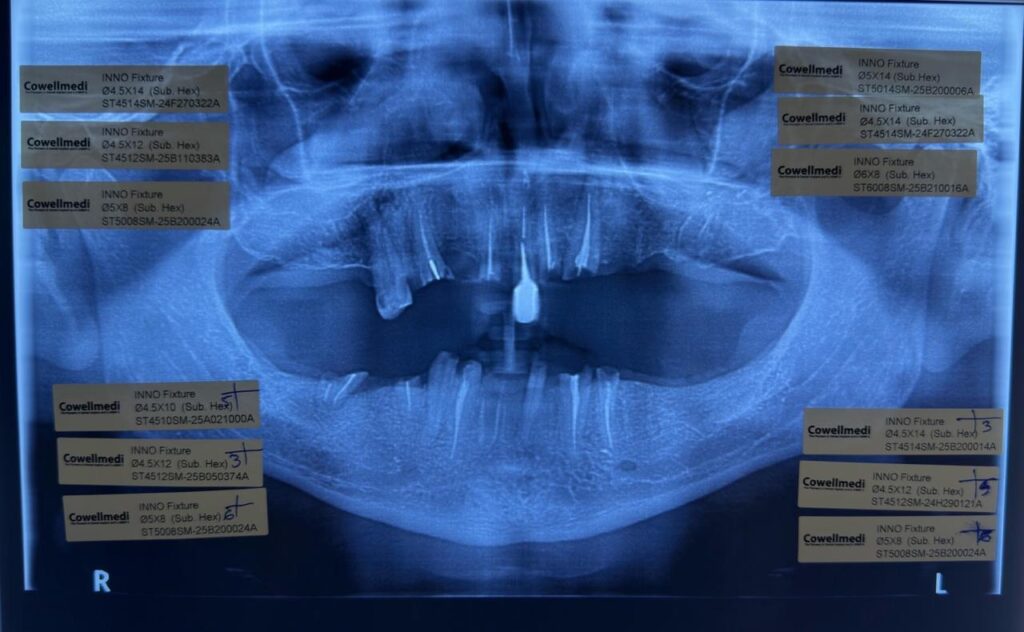
Thirteen extractions, 12 immediately placed dental implants across two surgical sessions, infection fully managed, and a fitted temporary prosthesis delivered before departure.
This post documents exactly what happened, the clinical decisions made at each stage, and what patients facing similar situations can realistically expect from full mouth implant rehabilitation.
Shams Raza Syed
“This review is for every Pakistani Expat out there or locals considering dental implants globally. Please read this before making your decision.”
“This review is for every Pakistani Expat out there or locals considering dental implants in Canada, Turkey, Mexico, Argentina — or anywhere else — and comparing multiple quotes. Please read this before making your decision.”
My name is Shams Raza Syed, I’m 47 years old, and I live in Toronto, Canada. I needed a major dental procedure: 6 upper implants and 6 lower implants. This was a huge decision — medically, financially, and emotionally. Like many of you, I spent months researching, comparing clinics, watching videos, reading reviews, and trying to understand who I could trust with something this important.
My selection criteria
- Highly experienced and educated implantologist
- Proven success rate (ideally close to 98%)
- Genuine patient reviews on Google and other platforms
- Transparent and affordable pricing
- A proper office setup with trained staff
- A functioning LaForme device to sterilize handpieces
I explored options globally — Canada, Turkey, Mexico, Argentina — and checked Pakistan almost as a coincidence. But during my search for the top implantologist in Karachi with strong credentials, real experience, recognized certifications, a reputable name, and an active presence on YouTube and Instagram, I came across Dr. Saqib Minhas in Gulshan E Iqbal.
And that changed everything.
Unlike many dentists who do a quick glance and move on, Dr. Saqib took his time. He carefully examined my mouth, reviewed my X‑rays in detail, and prepared a clear, well‑thought‑out treatment plan tailored specifically to my case. His approach was methodical, precise, and rooted in deep expertise.
Day 1 — May 5th, 2026 (Lower Jaw)
I went in for 6 lower‑jaw implants and 6 extractions. From start to finish, the experience was incredible.
- He checked my blood pressure every 30 minutes, ensuring I was stable and comfortable.
- He constantly communicated, explaining each step as he worked.
- He kept me calm with genuine, reassuring conversation, not rushed or forced.
I had an infection on my lower right side, and instead of rushing, he spent an extra 50 minutes carefully cleaning, disinfecting, and repairing the area. No shortcuts. No compromises.
The lower‑jaw procedure took 5 full hours — and every minute was focused, detailed work. At one point, we were going past our scheduled time, and I must have looked concerned. He paused, looked at me, and said something I will never forget:
“Don’t worry. We are here even if we have to work till 2 am. We aren’t going anywhere and we aren’t rushing through this. We will take as long as it takes.”
That level of dedication is rare anywhere in the world.
Day 2 — May 6th, 2026 (Upper Jaw)
The next day, I returned for the upper‑jaw implants. Another 5 hours of focused, meticulous work.
Total Extractions
14
Total Implants
12
Surgery Time
10+ hrs
What truly stood out
After placing each implant, he took an X‑ray immediately to confirm perfect positioning. That level of precision and accountability is something I have never seen before — and it gave me complete confidence in the implants he placed.
He also ensured that each implant was placed deep and correctly into the bone, which is absolutely critical for long‑term success. This is the kind of detail that separates a good implantologist from a world‑class one.
The clinic itself
His clinic is modern, clean, and equipped with the technology you expect from top-tier international dental centers. His staff is professional, kind, and well-trained. The environment immediately gives you the sense that you’re in the right hands.
If you’re comparing global options or considering dental tourism, put Pakistan — and specifically Dr. Saqib Minhas — on your list. You get world-class expertise, transparent pricing, and a level of care that is hard to find anywhere else.
For anyone researching, worrying, or overthinking like I was: You owe it to yourself to consult with Dr. Saqib Minhas before making your final decision.
Full mouth implant rehabilitation is possible even when all teeth are non-restorable and infection is present. With proper surgical sequencing and infection management, immediate implant placement can be performed safely. The process typically involves two treatment phases: surgery and temporary prosthetics first, followed by final implant-supported teeth after the implants have fully integrated with the bone.
The Patient’s Condition When He Found Us
The patient had conducted extensive research internationally before selecting The Dental Clinic in Karachi for treatment. When he arrived, clinical and radiographic examination confirmed what he already suspected: there was nothing left to save.
The examination found multiple badly decayed roots throughout both the upper jaw (maxilla) and lower jaw (mandible). A badly decayed root, or BDR, is what remains when a tooth has deteriorated to the point where it can no longer be restored with a crown or any other restorative option.

The patient had only one remaining standing tooth, and even that had been rebuilt using a dowel crown, a post placed inside the root to support an artificial crown on top.
Active infection was present at multiple sites. Bone quality and quantity were assessed carefully to determine whether immediate implant placement was viable.
Why All Teeth Had to Be Removed
Patients often ask whether there is any alternative to full extraction in cases like this. In this patient’s situation, the answer was no.
When teeth are classified as non-restorable, it means the remaining tooth structure, root included, cannot support any form of restoration. Attempting to keep non-restorable teeth in place leads to continued bone loss, spreading infection, and implant failure if implants are eventually placed adjacent to compromised roots. Removing all non-restorable teeth and roots is not just the recommended path in cases like this; it is the only clinically sound one.

The presence of infection made extraction timing and sequencing especially important. Each site had to be thoroughly debrided, meaning cleaned of infected tissue and debris, before any implant could be placed.
The Treatment Plan
The clinical team developed a plan to complete full-mouth extraction and immediate implant placement across two consecutive surgical sessions, one for the lower arch and one for the upper arch. A temporary removable denture would be fabricated before the patient returned abroad, giving him functional teeth throughout the healing period.
| Phase | Timing | What Was Done |
|---|---|---|
| Assessment | Pre-surgery | Clinical exam, full X-rays, bone and infection evaluation, treatment planning |
| Lower arch surgery | Day 1 | All lower teeth and roots removed, infection cleared, 6 implants placed, X-ray verification |
| Upper arch surgery | Day 2 | All upper teeth and roots removed, sites cleaned, 6 implants placed, X-ray verification |
| Healing reviews | Post-surgery | Multiple follow-up visits during recovery |
| Prosthetics | Pre-departure | Temporary denture delivered and adjusted |
Day 1: Lower Arch Surgery
On the first surgical day, all non-restorable lower teeth and roots were removed. This alone is a significant procedure. The lower arch in this patient required removal of multiple roots that had fractured at or below the gum line, which demands precise technique to avoid damaging the surrounding bone.
Once extractions were complete, each socket was debrided to eliminate infected tissue and prepare a clean environment for implant placement. Bone preparation followed, shaping the implant sites to receive the titanium implants at the correct angles and depths.
Six mandibular implants were then placed immediately into the prepared sites. Intraoperative X-rays were taken to verify that each implant was correctly positioned before the patient left the chair.


Why Immediate Placement Rather Than Waiting
A common question is whether it is safer to wait for extraction sites to heal before placing implants. In selected cases, immediate placement after extraction offers real advantages: it reduces the total number of surgical procedures, helps preserve bone volume at the extraction site, and compresses the overall treatment timeline.
Research supports immediate implant placement as a predictable approach when infection is properly managed and bone quantity is adequate. In this patient’s case, the thorough debridement performed during extraction made immediate placement clinically appropriate.
Day 2: Upper Arch Surgery
The second surgical session followed the same protocol for the upper arch. All remaining non-restorable maxillary teeth and roots were removed, infected tissue was cleared, and implant sites were carefully prepared.


Six maxillary implants were placed and their positions were confirmed radiographically before the session ended. At this point, the patient had 12 dental implants placed across both arches within a 48-hour window.

Post-Operative Care and the Temporary Prosthesis
Following surgery, the patient was reviewed multiple times during his recovery period. These visits allowed the clinical team to monitor tissue healing, check for any signs of complication, and adjust care as needed.
Before the patient returned abroad, a temporary removable denture was fabricated and fitted. This is not a permanent solution; it is a carefully constructed interim prosthesis designed to restore appearance and basic function while the implants undergo osseointegration, the process by which the titanium implant fuses with the surrounding jawbone.
Adjusting the Temporary Denture

The temporary denture required several chairside adjustments before it was ready. The team refined the occlusion, meaning the way the upper and lower teeth meet when biting, and relieved pressure areas to prevent soreness during healing.
Aesthetic adjustments were also made so the patient would feel comfortable and confident during his time abroad.
The patient departed with a denture that fit well, looked natural, and allowed him to eat and speak with reasonable comfort.
Clinical Outcome
Recovery was uneventful. There were no reported surgical complications, and the patient’s tissue response was described as appropriate throughout the healing reviews.
At the conclusion of Phase 1, the patient reported high satisfaction across every aspect of his care: the clarity of the treatment plan, the precision of the surgery, the management of his infection, the communication he received throughout, the quality of follow-up, and the fit and appearance of his temporary denture.

The patient is now in the osseointegration phase and is scheduled to return to The Dental Clinic for Phase 2, when the final implant-supported prosthesis will be designed, fabricated, and fitted. Read patient reviews and experiences https://maps.app.goo.gl/FzDSdwvQ4EJc2LoS8?g_st=iw
Frequently Asked Questions
Yes, in many cases. Immediate implant placement, meaning placing the implant into the extraction socket on the same day the tooth is removed, is a well-established technique. It works best when there is adequate bone volume, the site can be thoroughly cleaned of infection, and the implant can be placed with good primary stability.
Active infection does not automatically rule out implant placement, but it requires careful management. The infected tissue must be fully removed and the site debrided before the implant is placed. Leaving residual infection in an implant site is a common cause of early implant failure.
Implant-supported prostheses are designed to replicate the look, feel, and function of natural teeth as closely as possible. Unlike removable dentures, implant-supported teeth are anchored into the jawbone, which means they do not shift or require adhesives. Patients can eat, speak, and smile normally. The final prosthesis in a full-arch case is custom-designed to match the patient’s facial structure and aesthetic preferences.
Get Expert Dental Care at The Dental Clinic
For patients in Karachi and those traveling from abroad, The Dental Clinic offers the surgical expertise and treatment infrastructure needed for complex full-mouth rehabilitation cases. The clinic’s approach combines thorough pre-surgical planning with precise execution, giving patients a clear picture of what to expect before treatment begins and a well-supported recovery after it ends.
Dr. Saqib Minhas leads implant cases at The Dental Clinic with a focus on long-term outcomes. Cases involving full-arch extractions, immediate implant placement, and active infection management require both surgical skill and sound clinical judgment. Dr. Minhas brings that experience to every full-mouth rehabilitation case the clinic undertakes.
If you are dealing with failing teeth, non-restorable roots, or have been told elsewhere that your options are limited, a consultation at The Dental Clinic is the right starting point. Visit thedentalclinic.com.pk to book your assessment and find out what is possible for your specific situation.